Mission / Purpose
Straight Healthcare's primary mission is to provide comprehensive, concise, evidence-based medical information. Healthcare evolves rapidly, inundating providers with new studies, drugs, and guidelines that must be integrated into their practices. Spiraling healthcare costs are often driven by treatments and interventions with no proven benefit. Conscientious providers must equip themselves with the best information available to make confident recommendations in an ever-expanding world of expensive treatments and diagnostic modalities.
Hundreds of medical studies are published every month, as computer advances and healthcare databases have made it possible to evaluate large amounts of data with little effort. It's more important now than ever that providers understand the principles of quality medical research and sound statistical techniques so they can decipher which information will improve their outcomes.
Written from a primary care perspective, Straight Healthcare strives to analyze and present the best information available so everyone can make informed healthcare decisions.
Developer / Author
Dr. Todd Crump has a Bachelor of Science in Pharmacy from The University of Texas at Austin and a Doctor of Medicine from The University of Texas Health Science Center in San Antonio. He is board-certified in family medicine and is a registered pharmacist.
Why I became interested in evidence-based medicine
Healthcare is humbling. I've missed obvious diagnoses, overlooked drug interactions that landed patients in the ER, and felt inadequate more times than I like to admit. We all make mistakes, and medicine is complex, creating a rift between our desire to appear steadfastly competent and reality. For years, I never picked up a medical journal, relying heavily on what I learned in residency or saw other physicians doing. This approach helped me get through the grind of daily clinic but did little to appease my insecurities or stimulate me professionally. Feeling burned out, I sought ways to reengage, eventually discovering evidence-based medicine and my attempt to organize it with Straight Healthcare.
Evidence-based medicine provides a foundation for a systematic approach to diagnosing and treating patients. Knowing the information from the ground up, i.e., published studies, removes doubt, increases understanding, and decreases reliance on third-party guidance, which is often biased or based on a cursory review of the evidence. It also requires a deeper understanding of study design and statistical theory so that the evidence can be scrutinized and its true value extracted.
Straight Healthcare provides the necessary tools to treat patients from an evidence-based approach, including concise reviews of pivotal studies, professional guidelines, diagnostic algorithms, and drug information organized in an intuitive format. To learn more, explore our features below.
Watching the Grey Cup with my Canadian mail-order bride
Yoshi
Want to learn more about how Straight Healthcare helps make providers more efficient and knowledgeable? Take a tour of our features below.
Medication pages
Large medication classes organized in practical formats for quick access to relevant information and easy comparisons
Drug mechanism explained for better recall and understanding
Concise prescribing information
Concise prescribing information with important details like recommended lab monitoring, links to recent studies, and available dosage forms across brands
Study information
Pivotal and practice-changing studies presented in a concise format for easy interpretation. The example below is from our SGLT2 inhibitor page.
RCT
EMPEROR-Preserved trial - Empagliflozin vs Placebo in Heart Failure with Preserved Ejection Fraction, NEJM (2021) [PubMed abstract]
The EMPEROR-Preserved trial enrolled 5988 patients with NYHA class II - IV heart failure and an EF > 40%
Main inclusion criteria
NYHA class II - IV heart failure
EF > 40%
NT-proBNP level > 300 pg/ml (> 900 pg/ml if has A fib)
BMI < 45
Main exclusion criteria
MI, CABG, CVA within 90 days
Cardiac resynchronization therapy
SBP ≥ 180 mmHg
A fib with rate > 100 bpm
Baseline characteristics
Average age 72 years
Average BMI - 30
Average EF - 54%
Median NT-proBNP - 995 pg/ml
Diabetes - 49%
A fib - 51%
Ischemic heart failure - 35%
NYHA class: II - 81% | III - 18% | IV - <1%
Randomized treatment groups
Group 1 (2997 patients): Empagliflozin 10 mg once daily
Group 2 (2991 patients): Placebo
Primary outcome: Composite of adjudicated cardiovascular death or hospitalization for heart failure, analyzed as the time to the first event
Results
Duration: Median of 2.2 years
Outcome
Empagliflozin
Placebo
Comparisons
Primary outcome
13.8%
17.1%
HR 0.79, 95%CI [0.69 - 0.90], p<0.001
Heart failure hospitalization
8.6%
11.8%
HR 0.71, 95%CI [0.60 - 0.83]
Cardiovascular death
7.3%
8.2%
HR 0.91, 95%CI [0.76 - 1.09]
Overall mortality
14.1%
14.3%
HR 1.0, 95%CI [0.87 - 1.15]
Hypotension
10.4%
8.6%
N/A
UTI
9.9%
8.1%
N/A
Genital infections
2.2%
0.7%
N/A
Bone fractures
4.5%
4.2%
N/A
Lower limb amputations
0.5%
0.8%
N/A
Ketoacidosis
0.1%
0.2%
N/A
In subgroup analysis, the effects of empagliflozin on the primary outcome were similar in patients with or without diabetes
One year after randomization, the average decrease from baseline in SBP was 1.8 mmHg for empagliflozin and 0.6 mmHg for placebo (diff 1.2 mmHg, 95%CI [-2.1 to -0.3])
Findings: Empagliflozin reduced the combined risk of cardiovascular death or hospitalization for heart failure in patients with heart failure and a preserved ejection fraction, regardless of the presence or absence of diabetes.
Information on study design and interpretation
The excerpt below is from our Medical Studies page, where we review study types and methods, biases, confounding, and more. If you want to learn more about study interpretation and critique, check out our Medical Study Analysis CME.
AS-TREATED ANALYSIS
Overview
In an as-treated analysis, subjects are counted toward the therapy they actually received, meaning people assigned to treatment A who crossover to treatment B are counted toward treatment B. This differs from intention-to-treat analysis, where crossovers count toward their original assigned group, and per-protocol analysis, where crossovers are excluded.
As-treated analyses are often performed in studies with high crossover rates, and on the surface, they seem to be a logical way to handle crossovers. However, they are very prone to bias (see example below).
Example
Researchers want to compare surgery to physical therapy for sciatic nerve pain, so they randomize 200 patients with sciatica to physical therapy or surgery. The primary outcome is back pain and disability at one year.
Over the course of the study, 30 people assigned to physical therapy end up receiving surgery, and 10 people assigned to surgery never have surgery and instead receive physical therapy (crossovers)
The researchers decide to do an as-treated analysis so that crossovers count toward the therapy they received
Bias in as-treated analyses
In this example, results from 30 people in the physical therapy group are counted toward surgery, and results from 10 in the surgery group are counted toward physical therapy. This appears logical since the outcomes for crossovers now count toward the treatment they received. In reality, the analysis is likely biased. People often enter trials because they hope to receive one of the treatments being offered. Researchers know this, so they allow crossovers to boost enrollment. In the example above, patients who believe invasive treatments are better may be disappointed if they are assigned to physical therapy. They are biased toward surgery, and if they cross over, the as-teated analysis will also be biased. Another potential source of bias is the 10 subjects who did not receive surgery and counted toward physical therapy. It's possible these patients were sicker, making them poor surgical candidates. Applying their results to physical therapy shifts the balance of debilitated patients to one side.
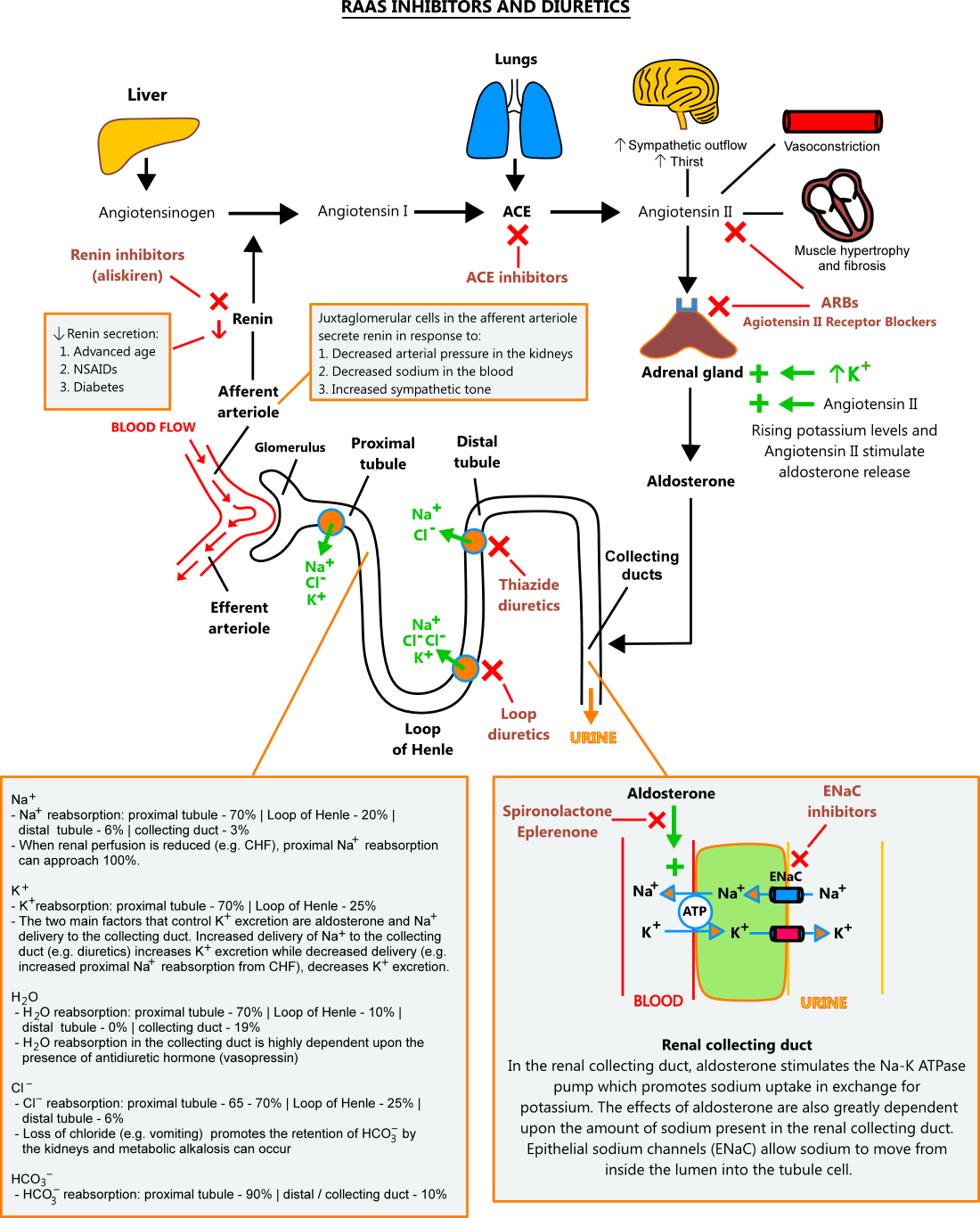
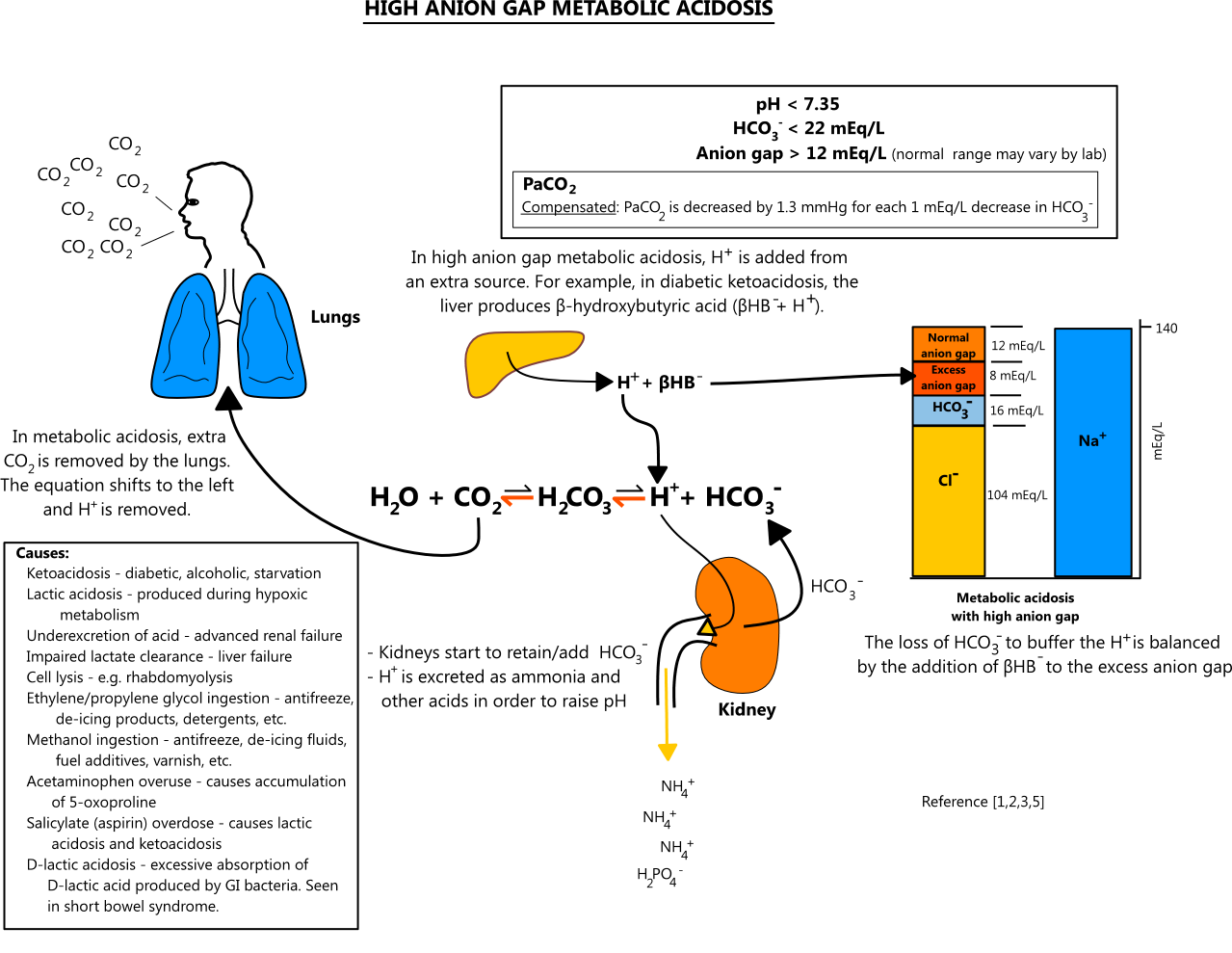
Physiology
Physiologic processes explained for better understanding and recall
Step-by-step diagnostic approaches to common abnormalities
The guidance below is from our Liver Tests and Diseases page
Mild ALT / AST Elevations (<5 X ULN)
Step 1 - assess patient
Assess for hepatotoxic prescription medications, OTC medications, supplements, and alcohol use (see the NIH Livertox Database for hepatotoxicity information on a large number of medications and supplements)
Assess risk factors for fatty liver (obesity, diabetes, dyslipidemia, hypertension)
If a hepatotoxic drug or supplement is identified, consider discontinuing the drug/supplement and rechecking enzymes in 6 weeks
If patient consumes regular alcohol, recommend alcohol cessation and recheck enzymes in 6 weeks
If patient is overweight, recommend weight loss and recheck at later date, keeping in mind that significant weight loss is difficult for most people to achieve
Step 2 - initial workup
CBC with platelets
Liver testing including ALP, bilirubin, and albumin
PT/INR
Hepatitis panel (should include HBsAg, HBcAb, HBsAb, HCV Ab)